Skip to main content
Skip to main content

 01274 442076
01274 442076





PCN Cancer Screening: How to Meet DES Expectations
|
Getting your Trinity Audio player ready...
|
PCNs must deliver measurable improvements in PCN cancer screening uptake, to meet the 2026/27 Network Contract DES. Moving beyond simple awareness to targeted, data-led delivery. For PCN leaders, this means operationalising breast, bowel, and cervical screening requirements while integrating new mandates for lung cancer screening and reducing inequalities.
- What does the DES require from PCNs on cancer screening in primary care?
- Which screening programmes should PCNs focus on?
- How can PCNs improve screening uptake without overloading practices?
- What role does data play in reducing cancer screening inequalities?
- How should PCNs identify and manage non-responders?
Key Takeaways
- Contractual Mandate: The 2026/27 DES explicitly requires PCNs to improve screening uptake, with a focus on non-responders and deprived populations.
- Operational Clarity: New requirements for referral quality (aligned with NICE Guideline 12) and electronic safety-netting provide a clearer framework for delivery.
- Funding Support: A new £200 million national fund is available to tackle cancer screening inequalities in deprived areas, supporting local outreach and data-led interventions.
- Expanded Scope: PCNs must now also engage with the Lung Cancer Screening Programme, sharing data to support its national rollout.
What does the DES require from PCNs on cancer screening in primary care?
The Network Contract DES for 2026/27 mandates that PCNs work with partners to improve the uptake of breast, bowel, and cervical screening. This is no longer a “best efforts” activity; PCNs must demonstrate proactive work to identify and support eligible patients who have not responded to initial invitations. The specification also introduces stricter requirements for referral quality, ensuring that all suspected cancer referrals meet the criteria set out in NICE Guideline 12.
Which screening programmes should PCNs focus on?
While the core focus remains on the three national screening programmes (breast, bowel, and cervical), the 2026/27 contract introduces a formal requirement to support the NHS Lung Cancer Screening Programme. PCNs are expected to share data and facilitate the identification of eligible individuals for lung health checks. This expansion reflects the broader NHS goal of early cancer diagnosis in PCNs, where screening plays a pivotal role in shifting from late-stage treatment to early-stage intervention. For a wider overview of what is health screening, including how NHS programmes are structured, see our guide.
How can PCNs improve screening uptake without overloading practices?
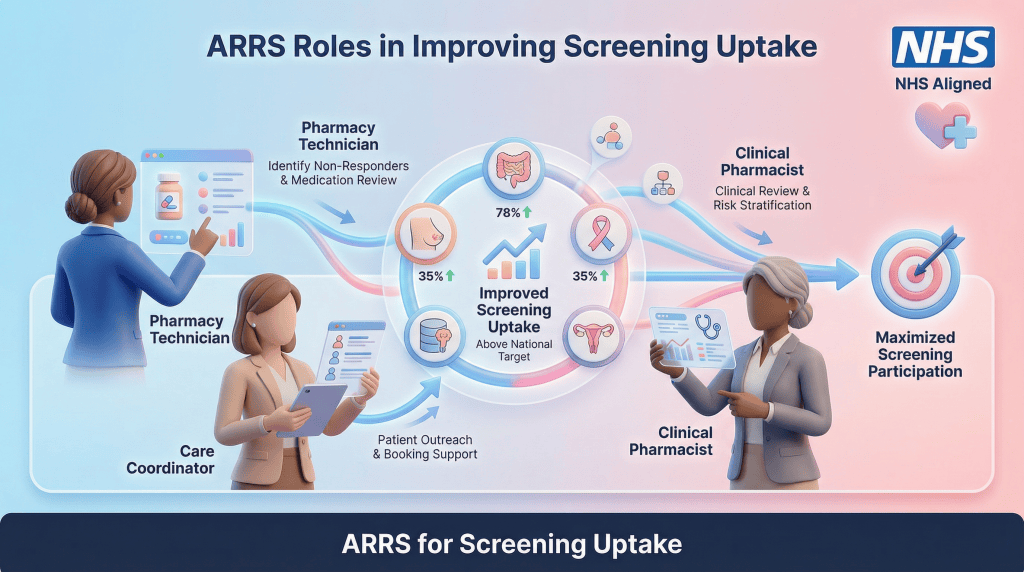
Improving uptake requires a centralised, PCN-level approach rather than adding burden to individual practices. Utilising the Additional Roles Reimbursement Scheme (ARRS) allows PCNs to deploy Care Coordinators and Pharmacy Technicians to lead on data audits and patient outreach. By identifying non-responders through risk-stratification tools, PCNs can deliver targeted text reminders, phone calls, or even community-based clinics, ensuring that clinical staff can focus on high-complexity Structured Medication Reviews and acute care.
| ARRS Role | Contribution to Cancer Screening Uptake |
| Pharmacy Technician | Leads data audits, identifies non-responders, and supports safety-netting processes for NICE Guideline 12 compliance. |
| Care Coordinator | Manages “last mile” outreach, bridging the gap between data lists and patients attending appointments or returning kits. |
| Clinical Pharmacist | Provides clinical oversight, handles complex patient queries regarding screening, and integrates screening checks into routine reviews. |
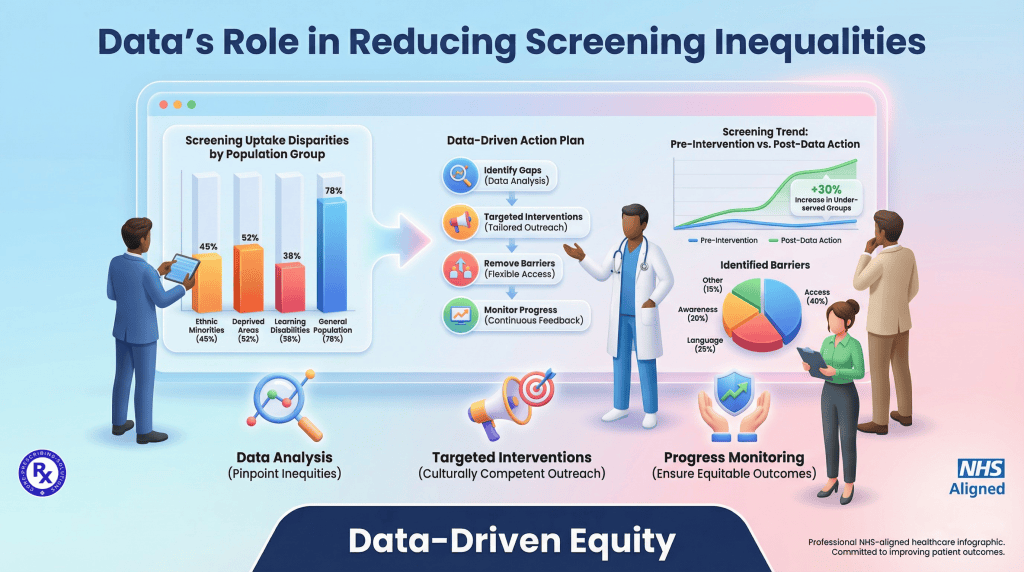
What role does data play in reducing cancer screening inequalities?
Data is the most powerful lever for reducing the “screening gap” in deprived areas. The need for measurable improvements is clear: in some deprived areas, bowel cancer screening uptake can be as much as 20% to 25% lower than in affluent areas, and cervical screening coverage for the 25-49 age group often hovers around 68% to 70% nationally, well below the 80% target. PCNs should use the Core20PLUS5 framework to identify populations at the highest risk of late diagnosis. By cross-referencing screening data with deprivation indices and ethnicity, PCNs can tailor their outreach. For example, providing information in multiple languages or offering evening screening appointments can significantly improve participation among groups that traditionally face barriers to access.
How should PCNs identify and manage non-responders?
PCNs must actively identify non-responders using screening data and implement targeted recall systems to improve uptake. This involves leveraging patient recall systems, developing proactive outreach methods, and integrating regular audit cycles to monitor and improve performance. By systematically addressing non-response, PCNs can significantly boost overall screening rates and reduce health inequalities.
PCNs improve screening uptake by:
- Identifying non-responders through data audits
- Using targeted recall systems
- Delivering community outreach
- Monitoring performance through regular audit cycles
Expert insight from Adeem Azhar, qualified Clinical Pharmacist and CEO
The shift towards operational accountability in the 2026/27 DES is a significant step. PCNs that leverage their multidisciplinary teams to lead on screening uptake will not only meet their contractual obligations but, more importantly, save lives through earlier cancer diagnosis.
Adeem Azhar, MPharm, IPres
Co-Founder and Chief Executive Officer – Core Prescribing Solutions
Qualified Clinical Pharmacist
FAQs
Looking for support with your PCN cancer screening delivery?
If your PCN needs help operationalising the 2026/27 DES requirements, we can support you. Our clinical teams and data specialists integrate with your PCN to drive screening uptake and ensure compliance with early cancer diagnosis targets.