Skip to main content
Skip to main content

 01274 442076
01274 442076





Combining SMRs with CVD Prevention to Meet QOF Targets Efficiently
|
Getting your Trinity Audio player ready...
|
QOF hypertension indicators remain a high-value area in 2026/27 following the CVD-focused changes introduced in 2025/26, making cardiovascular disease (CVD) prevention a key priority for both income and patient outcomes in primary care. For Primary Care Networks (PCNs), the challenge is improving these metrics without adding extra clinics. Structured medication reviews (SMRs) provide a practical solution, bringing blood pressure optimisation, lipid management, and safer prescribing into a single, targeted workflow.
- What are the QOF hypertension indicators for 2026/27?
- How do structured medication reviews support CVD prevention?
- What does a treatment to target pathway look like in practice?
- How does statin optimisation fit within the same review?
- How does this approach support safer medicines optimisation and workload efficiency?
Key Takeaways
- Higher QOF value: QOF hypertension indicators are worth significantly more points in 2026/27.
- Combined workflow: Structured medication reviews for long-term conditions combine CVD prevention and medicines optimisation.
- Active management: Treatment to target pathways ensure patients are actively moved toward BP and cholesterol goals.
- Reduced duplication: A combined SMR and CVD workflow reduces fragmented appointments and supports workload efficiency in primary care.
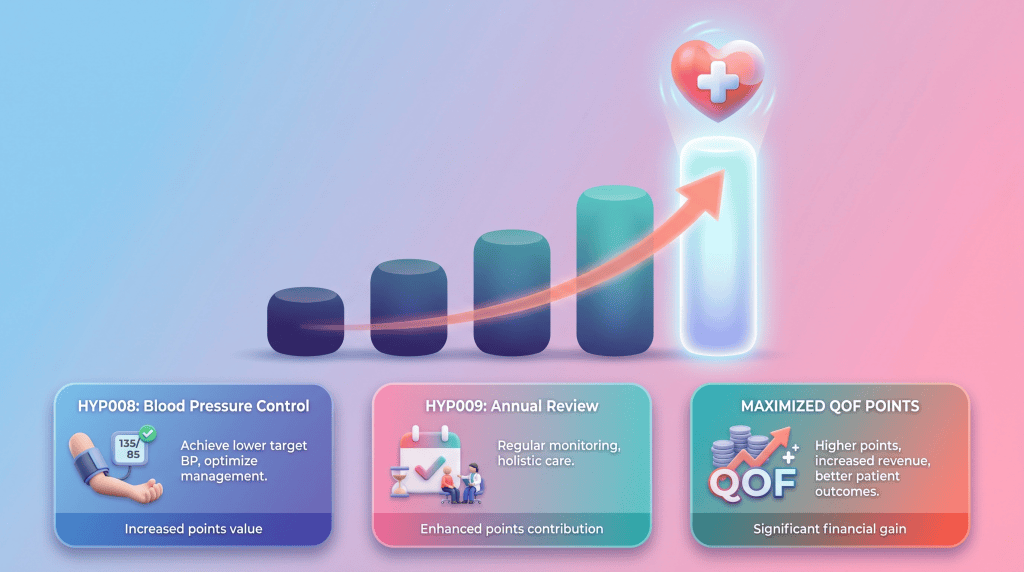
What are the QOF hypertension indicators for 2026/27?
Hypertension indicators are now highly valuable within the Quality and Outcomes Framework (QOF). The 2026/27 NHS England QOF guidance highlights two main targets: HYP010 (patients under 79 with BP ≤140/90 mmHg, worth 38 points) and HYP011 (patients aged 80+ with BP ≤150/90 mmHg, worth 14 points). Both indicators now have upper thresholds of 85%.
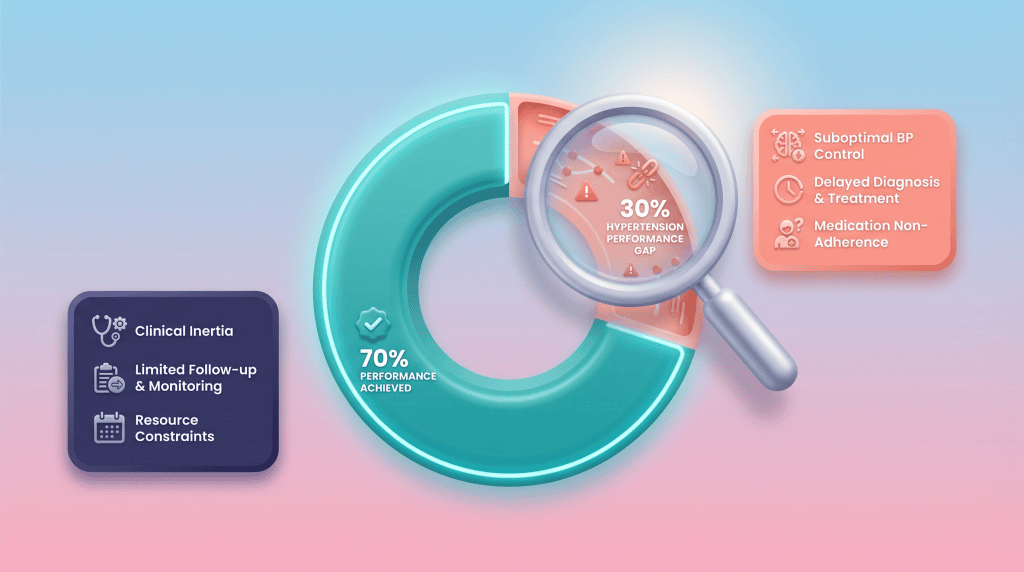
National data shows around 30% of patients with diagnosed hypertension are either not at target or lack a recent reading. This creates a substantial performance opportunity for practices to improve their QOF performance.
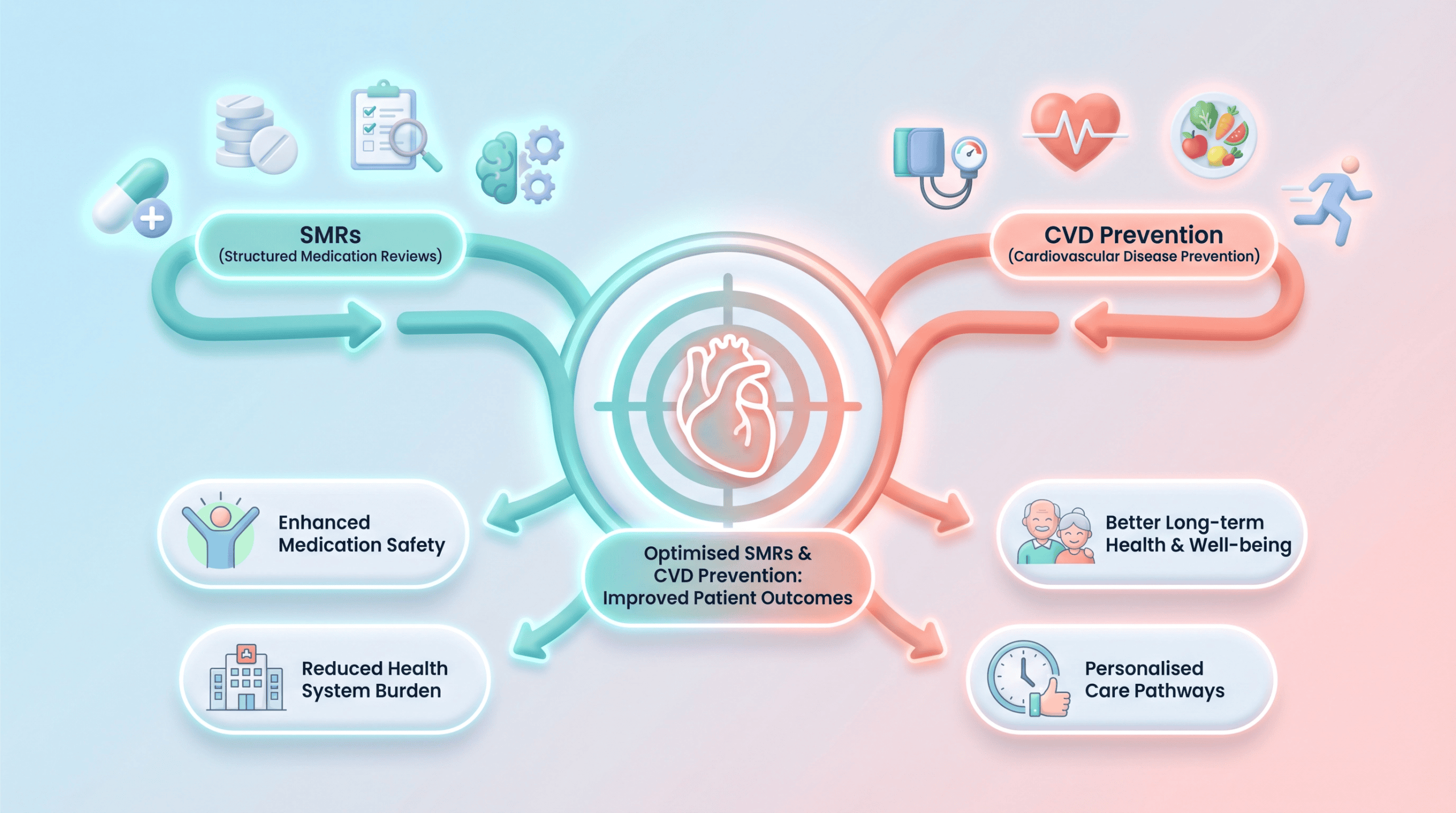
How do structured medication reviews support CVD prevention?
SMRs are designed for patients with long-term conditions, polypharmacy, or higher clinical risk. SMRs allow practices to prioritise patients with uncontrolled hypertension, those not on optimal lipid-lowering therapy, and individuals with adherence issues.
This makes structured medication reviews LTC a targeted intervention. SMRs are about making clinical decisions that improve outcomes and support effective long-term condition management.
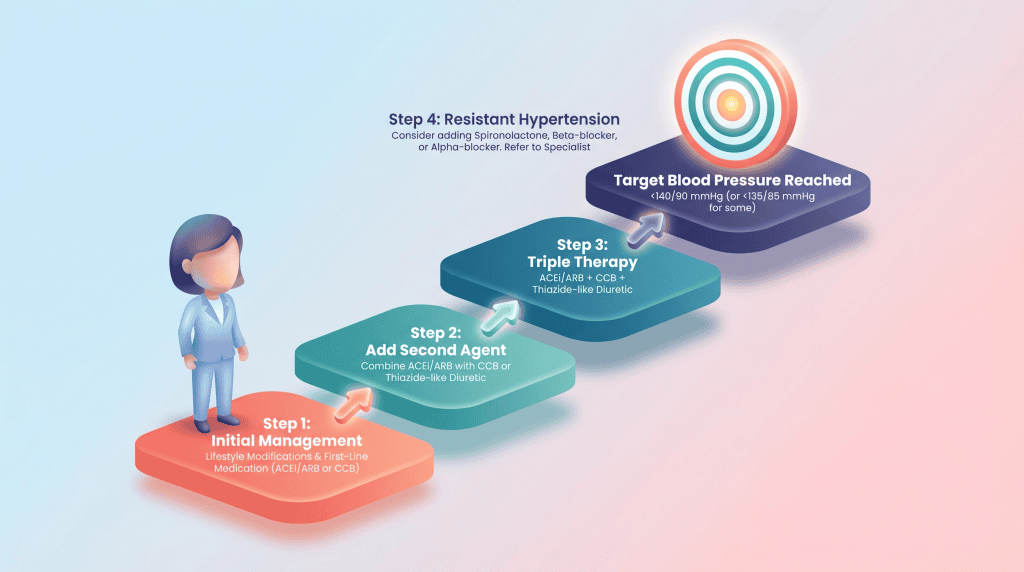
What does a treatment to target pathway look like in practice?
One of the biggest gaps in primary care is “clinical drift”- where patients remain above target without treatment being escalated. For hypertension, NICE guidance (NG136) recommends a stepwise approach to blood pressure treatment, with drug choice depending on the patient group and escalation based on adherence, tolerated doses and response.
An SMR provides the protected time to confirm adherence before escalation, assess tolerability, review home BP readings, and safely intensify treatment.
How does statin optimisation fit within the same review?
Cholesterol indicators are also heavily weighted in 2026/27. Within the same SMR, Clinical Pharmacists can identify patients not on any lipid-lowering therapy, review whether current statin optimisation therapy is appropriate, and address perceived intolerance.
For primary prevention, NICE NG238 recommends atorvastatin 20 mg for patients with a QRISK3 score of 10% or more. In practice, optimisation is based on response rather than a fixed cholesterol threshold, with NICE advising a greater than 40% reduction in non-HDL cholesterol. If this reduction is not achieved, and adherence is confirmed, treatment can be escalated safely.
How does this approach support safer medicines optimisation and workload efficiency?
CVD prevention must be done safely. SMRs support safer medicines optimisation by identifying high-risk prescribing, reviewing polypharmacy, assessing frailty, and ensuring appropriate monitoring.
Combining structured medication reviews with cardiovascular prevention allows practices to focus on the patients who will benefit most, improving outcomes while making better use of clinical time.
Adeem Azhar, Co-Founder and Chief Executive Officer – Core Prescribing Solutions
Instead of separate BP reviews and cholesterol clinics, practices can deliver one structured consultation. This is where workload efficiency in primary care improves-fewer fragmented appointments and more meaningful clinical interventions led by Clinical Pharmacists and supported by Pharmacy Technicians.
FAQs
Looking for support with your PCN clinical pharmacy workforce?
If your PCN wants to improve QOF performance through targeted structured medication reviews, we can help. Our Clinical Pharmacists and Pharmacy Technicians integrate with your team to deliver proactive cardiovascular care and medicines optimisation.