Skip to main content
Skip to main content

 01274 442076
01274 442076








What Does a Good ARRS Clinical Pharmacy Delivery Model Look Like?
28th February 2026
- Why Do Many PCNs Struggle With ARRS Delivery?
- What Should an ARRS Implementation Plan Include?
- How Should PCNs Measure ARRS Impact?
An effective ARRS clinical pharmacy delivery model in a PCN is a structured system that defines workforce roles, embeds supervision, standardises workflows, and measures outcomes. For PCN leaders, this means moving from reactive diary management to a predictable PCN pharmacy workforce model that improves safety and performance.
Key Takeaways
- Clear scope prevents drift: Defined roles reduce duplication and protect patient safety.
- Governance reduces risk: Formal supervision and escalation must be documented, not assumed.
- Workflows drive stability: Time-blocked clinics create consistent, predictable output.
- Measurement creates accountability: Reporting on outcomes, not just activity, demonstrates impact.
Why Do Many PCNs Struggle With ARRS Delivery?
Most ARRS workforce planning and PCN pharmacy workforce models fail because a clear structure is missing. While funding exists under the Additional Roles Reimbursement Scheme and expectations are set in the Network Contract DES, implementation varies significantly.
Common challenges include blurred role boundaries, reactive diary filling, informal supervision, and reporting focused on activity rather than outcomes. If you are reviewing how your network deploys ARRS roles, our dedicated ARRS support service explains how structured workforce planning works at PCN level.
What Should an ARRS Implementation Plan Include?
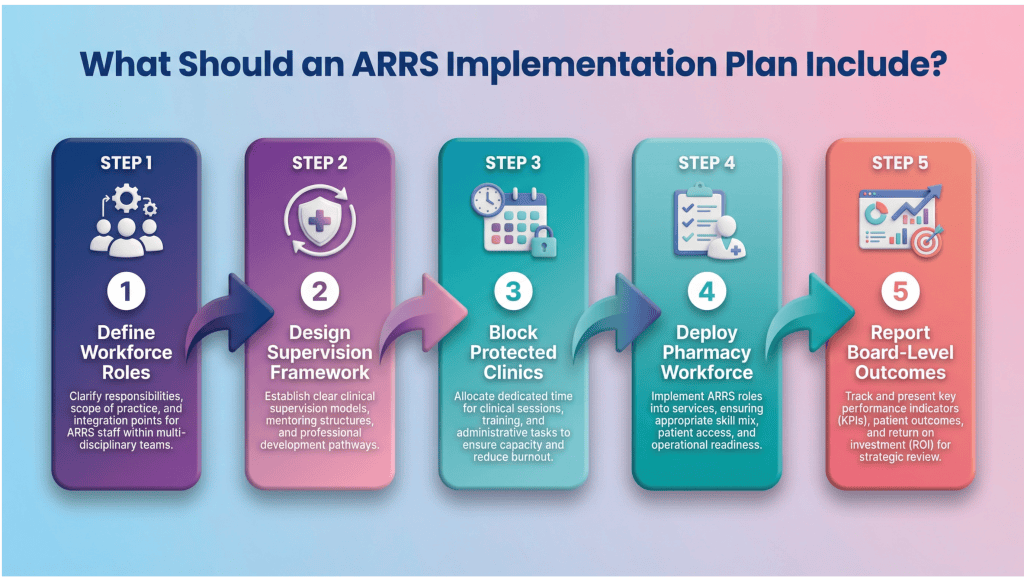
A strong ARRS implementation plan includes defined workforce roles, formal governance, repeatable clinics, and measurable KPIs. It should align with medicines optimisation principles from the National Institute for Health and Care Excellence. In practice, this rests on four pillars.
1. Clear Workforce Structure
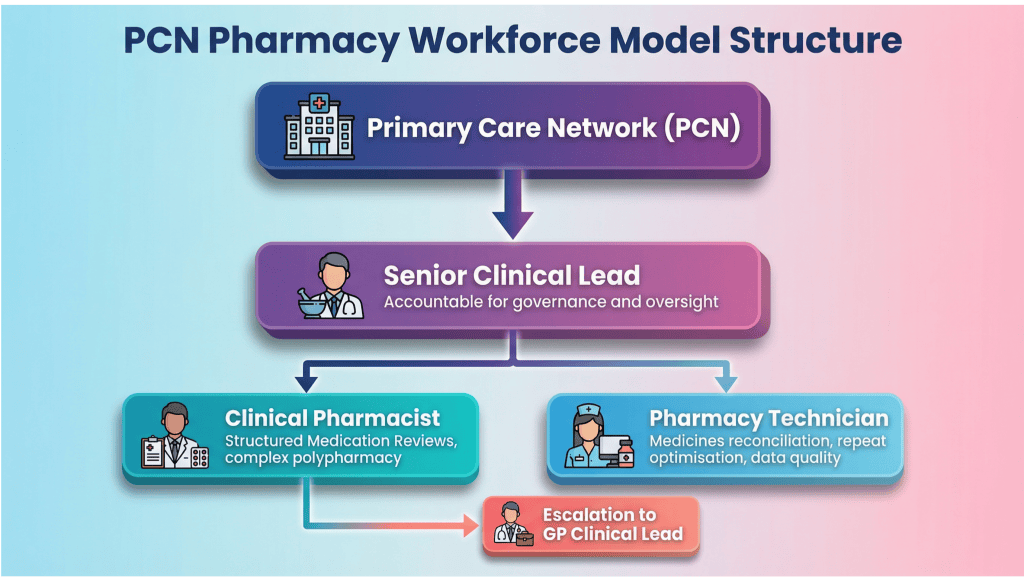
A safe ARRS delivery model starts with explicit role definition. Each role should have a documented scope of practice, defined boundaries, and a clear reporting line. This operationalises the intended design of the clinical pharmacy PCNmodel, clarifying the role of clinical pharmacists in PCNs and how they integrate with the wider practice team.
| Role | Core Responsibility | Boundary |
| Clinical Pharmacist | Structured Medication Reviews, complex polypharmacy | Escalates diagnostic uncertainty to GP |
| Pharmacy Technician | Medicines reconciliation, repeat optimisation, data quality | Does not independently alter complex therapy |
| Senior Clinical Lead | Supervision, governance oversight, prescribing risk review | Accountable for PCN-level pharmacy performance |
2. Structured Medication Reviews as the Clinical Anchor
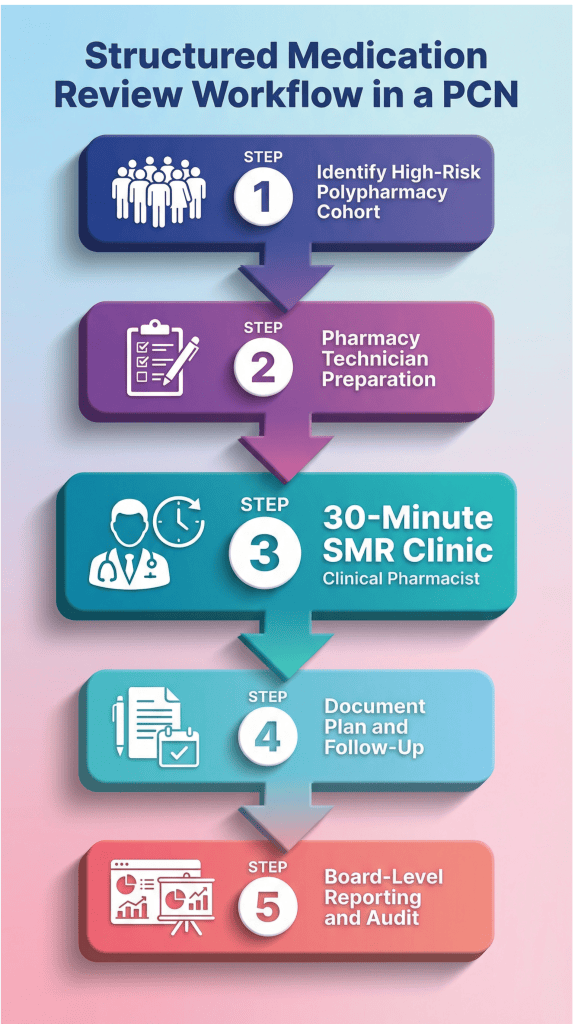
Structured Medication Reviews (SMRs) are the engine of most effective models. NHS England expects PCNs to prioritise high-risk patients for structured medication reviews PCN under the DES. Our approach to structured medication reviews ensures this process is proactive and measurable.
3. Defined ARRS Clinical Governance

Effective ARRS clinical governance makes supervision visible, documented, and accountable at PCN level. A strong model includes a named Senior Clinical Pharmacist, protected weekly supervision sessions, documented learning points, and defined escalation pathways to a GP lead. Governance should not rely on informal conversations; it must be structured, recorded, and reviewable.
4. Repeatable Workflows and Time Blocking
Predictable performance comes from structured scheduling. This supports safer prescribing and stronger medicines optimisation and is a core component of our wider clinical pharmacist services.
| Clinic Type | Lead | Frequency | Measured Outcome |
|---|---|---|---|
| SMR Clinic | Clinical Pharmacist | Daily blocks | % high-risk cohort reviewed |
| Post-Discharge Reconciliation | Pharmacy Technician | Daily task list | 72-hour completion rate |
| LTC Optimisation | Clinical Pharmacist | Weekly blocks | QOF performance |
When medicines ownership is explicit, performance stabilises. PCNs that define scope, supervision, and reporting move from reactive firefighting to predictable system delivery.
Adeem Azhar, Co-Founder and Chief Executive Officer – Core Prescribing Solutions
How Should PCNs Measure ARRS Impact?

ARRS impact should be measured using clinical and operational indicators defined at the outset of the ARRS implementation plan. A mature ARRS delivery model reports performance at board level against agreed KPIs, including SMR completion rates, reconciliation times, and prescribing safety trends. This moves the conversation from “how busy are we?” to “what has changed because of this workforce?”
FAQs
Looking for support with ARRS workforce planning?
If your PCN wants a structured ARRS delivery model that improves safety, governance, and measurable outcomes, our dedicated ARRS support service provides full workforce design and implementation support.