Skip to main content
Skip to main content

 01274 442076
01274 442076





Clinical use of magnesium: What Pharmacists and GPs Should Know
|
Getting your Trinity Audio player ready...
|
Magnesium is widely used in clinical practice to treat hypomagnesaemia, a condition frequently overlooked in primary care, particularly in patients on long-term PPIs or diuretics. Magnesium deficiency is usually defined as serum magnesium below 0.7 mmol/L, though local lab ranges vary slightly. Clinical pharmacists and GPs should know when to test, how to treat, and which drug interactions require magnesium monitoring in primary care to reduce the risk of arrhythmias and digoxin toxicity.
- When should magnesium levels be tested in primary care?
- Which medications cause hypomagnesaemia?
- How is hypomagnesaemia classified and managed?
- What are the key drug interactions with low magnesium?
- What monitoring is required during magnesium replacement?
- A simple approach to magnesium monitoring in primary care
Key Takeaways
- Check magnesium before and during long-term PPI use, especially with digoxin or diuretics (MHRA)
- Think magnesium if hypokalaemia or hypocalcaemia won’t correct
- Treat mild cases orally (10-24 mmol/day in divided doses); escalate severe or symptomatic cases for IV
- Review the cause (PPI necessity, diuretic type/dose, renal function) to prevent recurrence
When should magnesium levels be tested in primary care?
Magnesium testing should be considered in patients with symptoms such as muscle cramps, fatigue, or weakness, and routinely in those on medications associated with hypomagnesaemia.
The MHRA advises healthcare professionals to “consider measuring magnesium levels before starting PPI treatment and repeat measurements periodically during prolonged treatment”, particularly for patients also taking digoxin or diuretics. PPI-induced hypomagnesaemia is a recognised risk, especially after 12 months of continuous use.
Test magnesium when:
- Starting long-term PPI therapy (baseline)
- Reviewing patients on PPIs for more than 12 months
- Hypokalaemia or hypocalcaemia is not responding to replacement
- Patients on loop or thiazide diuretics report muscle cramps or fatigue
- Digoxin toxicity is suspected
Which medications cause hypomagnesaemia?
Several commonly prescribed medications can lower magnesium levels, making medication review important for identifying at-risk patients.
| Medication Class | Examples | Mechanism |
| Proton pump inhibitors | Omeprazole, lansoprazole | Impaired intestinal absorption |
| Loop diuretics | Furosemide, bumetanide | Increased renal excretion |
| Thiazide diuretics | Bendroflumethiazide, indapamide | Increased renal excretion |
| Aminoglycosides | Gentamicin | Renal magnesium wasting |
| Immunosuppressants | Tacrolimus, ciclosporin | Renal tubular effects |
For patients on long-term PPIs, consider whether continued use is clinically necessary. Where appropriate, H2 receptor antagonists such as famotidine may be considered.
How is hypomagnesaemia classified and managed?
Mild magnesium deficiency (0.5-0.7 mmol/L) is often asymptomatic or causes non-specific symptoms, while severe deficiency (<0.5 mmol/L) can cause tetany, seizures, and arrhythmias.
Mild hypomagnesaemia is managed with oral magnesium replacement therapy at 10-24 mmol/day in divided doses. Licensed options include magnesium aspartate sachets (10 mmol), magnesium citrate tablets (4 mmol), and magnesium glycerophosphate. Start low and increase gradually to minimise diarrhoea.
Severe hypomagnesaemia requires IV magnesium sulphate in hospital, with ECG and blood pressure monitoring.
Treatment should continue for 1-2 days after levels normalise, as intracellular stores take longer to replenish.
What are the key drug interactions with low magnesium?
Low magnesium increases the risk of magnesium and digoxin toxicity by enhancing myocardial sensitivity. Patients taking digoxin alongside PPIs or diuretics should have magnesium monitored, particularly if symptoms of toxicity occur.
Hypomagnesaemia also potentiates QT-prolonging drugs, increasing arrhythmia risk. This is particularly relevant with antiarrhythmics, some antipsychotics, macrolides, and fluoroquinolones.
Expert insight from Adeem Azhar, qualified Clinical Pharmacist and CEO
Magnesium is easy to overlook in routine practice, but for patients on long-term PPIs or diuretics, proactive monitoring can prevent serious complications. A simple blood test and medication review can make a real difference.
Adeem Azhar, MPharm, IPres
Co-Founder and Chief Executive Officer – Core Prescribing Solutions
Qualified Clinical Pharmacist
What monitoring is required during magnesium replacement?
Magnesium monitoring in primary care should focus on confirming response to replacement, identifying ongoing causes such as continued PPI use or renal losses, and preventing recurrence through medication review and deprescribing where appropriate.
- Confirming response to replacement
- Identifying ongoing causes such as continued PPI use or renal losses
- Preventing recurrence through medication review and deprescribing where appropriate
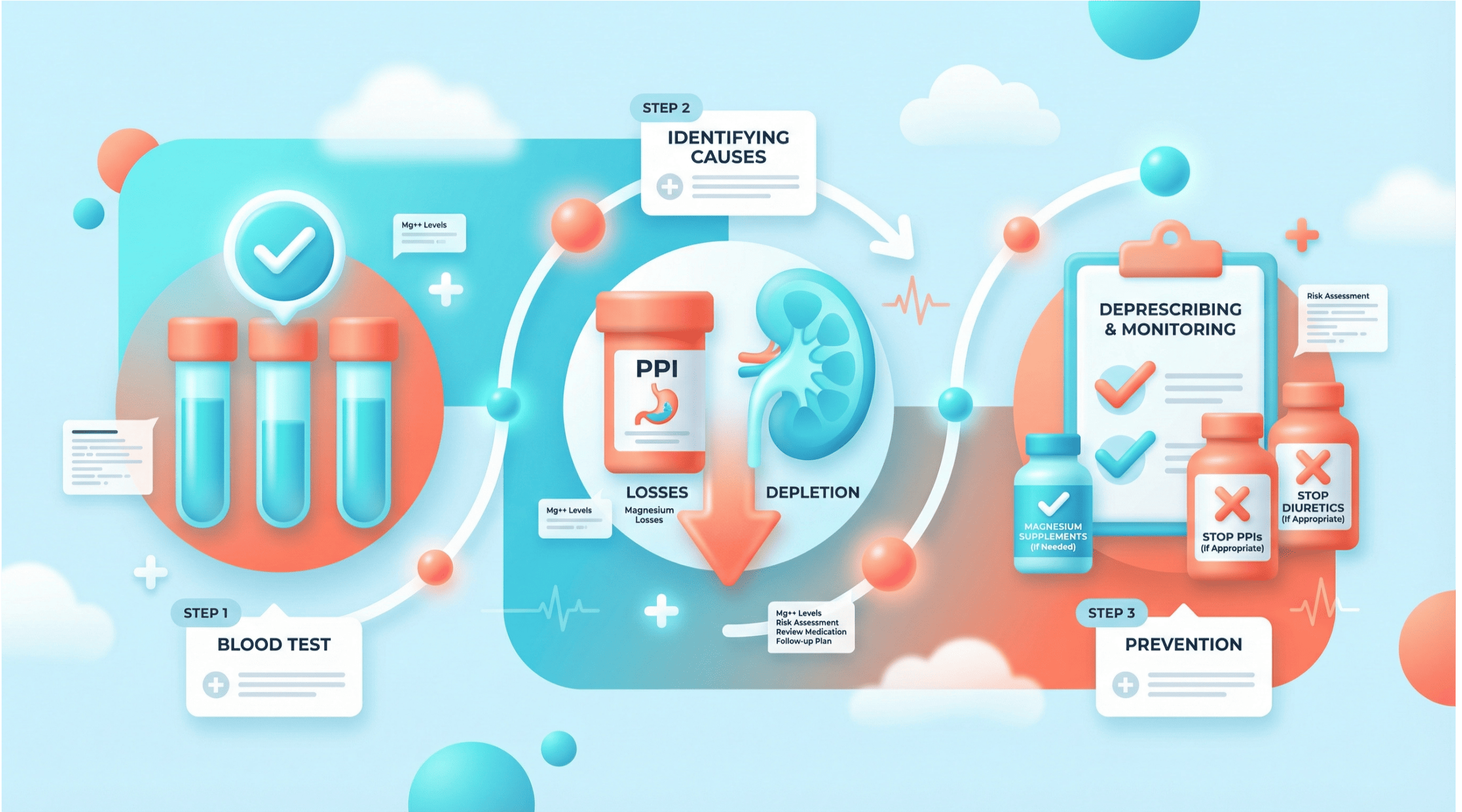
A simple approach to magnesium monitoring in primary care
- Baseline: Check magnesium before starting long-term PPI therapy
- At-risk patients: Repeat periodically in those on PPIs, diuretics, or digoxin
- After replacement: Recheck at 7 days, then at 1-3 months
- Ongoing risk: Review annually if the underlying cause persists
Recheck serum magnesium 7 days after starting oral treatment and again at 1-3 months depending on the cause. Monitor calcium and potassium, as deficiencies often coexist.
In patients with renal impairment (CKD 4-5, AKI, or dialysis), seek specialist advice before initiating replacement due to hypermagnesaemia risk.
FAQs
Need support with medication reviews?
If your practice or PCN needs additional capacity for structured medication reviews or long-term condition management, we can help identify patients at risk from long-term PPI or diuretic use and build monitoring into routine reviews.
For patients asking about over-the-counter supplements, including magnesium glycinate, see our guide to magnesium glycinate. For clinical guidance, refer to NHS SPS and the MHRA Drug Safety Update.